The fight against Antimicrobial Resistance:
A Global threat in Trauma and Orthopaedic surgery
An interview with:
— Professor. Chris Arts —
Issue 12, November 2024

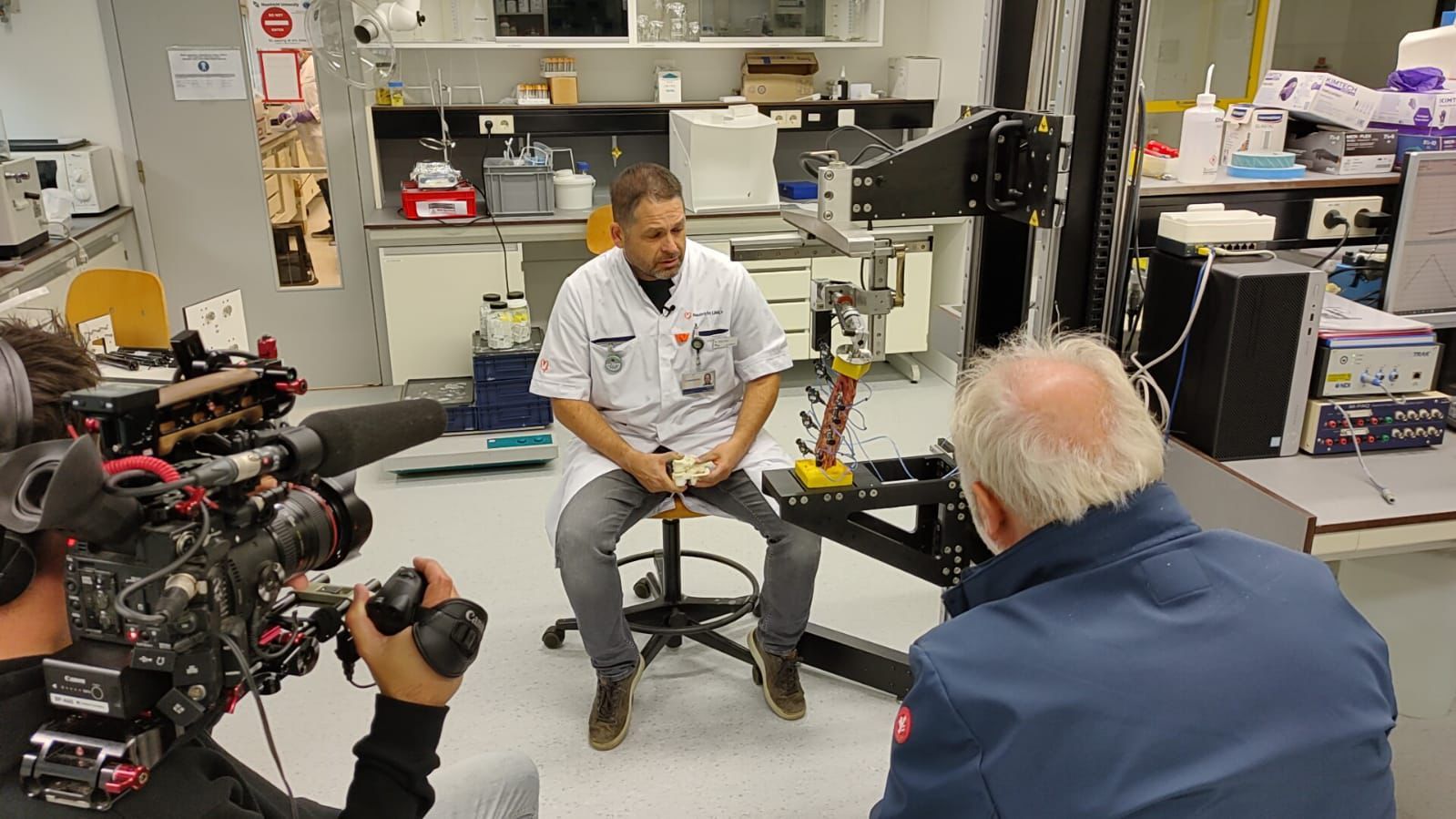
Can you tell us about your role as Professor of translational biomaterials at MUMC+ & TU/e?
Yes of course. I'm Professor of Translational Biomaterials at the Department of orthopaedic surgery at Maastricht University Medical Centre and at the research group for Orthopaedic Biomechanics at Eindhoven University of Technology. In addition I'm the project leader and principal investigator of the NWA DARTBAC consortium, where we collaborate with 26 partners to develop material technology to combat antimicrobial resistance and support infection treatment and prevention. I also act as project leader and principal investigator in a 14 partner Interreg project entitled Prosperos-II, where we develop personalised bioactive bone implants for patient functional recovery based on new workflows enabling statistical shape modelling, finite element modelling and in vitro and in vivo test models.
What is infection, and how does it present in Orthopaedics?
Orthopaedic infections are a group of infections that involve the musculoskeletal system, including bones, joints, and soft tissues. These infections can result from various causes, such as bacteria, viruses, or fungi, and can lead to complications like inflammation, pain, and impaired function. The incidence of infection in orthopaedic trauma patients is high, ranging from 5% to 10% depending on the location and severity of the injury, and the type of fracture. Infection in orthopaedic trauma patients is a common problem associated with significant financial and psychosocial costs, and increased morbidity.
How big is the problem of infection in orthopaedics
Depends on the country of course. Already in Europe, we observe distinct differences in infection incidence and recurrence rates. The Netherlands and Nordic countries that employ proper antibiotic stewardship, that restrict antibiotic prescriptions and also have a clean food and water supply are less impacted than southern European countries. For primary joint infection incidence it's about 1-2 percent, but after revision surgery most implant registries show that the incidence is creeping upward and also that the incidence of implant revision due to deep infection is increasing. In comparison to implants infection in high-energy trauma, open fractures or extensive spinal surgery its up to 55%
How do you see the limitations of antibiotics?
First of all they will become less effective due to antimicrobial resistance. Bacteria can and will adapt quickly to new environments and treatment therapies. In the short-term we can compensate for that by employing combination therapy, mixing antibiotics together or mixing antibiotics with known antimicrobial compounds such as silver or copper ions. In the long-term, new antibiotics are desperately needed, however big pharma companies are not invested in this partly because of the lack of return on investment and making a profit. The antibiotic development pipeline is underdeveloped at the moment. New reimbursement strategies or incentive schemes will help with that. Also, I firmly believe that repurposing medicine will yield new treatment options. Given these limitations, the DARTBAC project was started to develop material technologies to prevent bacterial attachment and biofilm formation on medical devices and in body tissues.

What drives your passion for infection and AMR?
First of all, I like to help patients. That is still my primary drive. Also, in infection prevention and treatment and also the development of new antimicrobial technologies and diagnostics, disciplines need to come together and I like working in a multidisciplinary setting. You can learn much from each other.
Can you tell us about DARTBAC?
DARTBAC is an interdisciplinary 26 partner consortium from academia, industry, health funds, Dutch Institute of Heath and the Environment (RIVM) and communication partners that focuses on antimicrobial resistance (AMR) awareness within the Netherlands and Europe and the development of new material technology and diagnostics for prevention and treatment of infectious diseases. In our development of material technologies we work on additive manufacturing for implant surface modification, bioactive peptides, bioactive coatings, bioactive glass bacteriophages,induction heating and radiopharmaceuticals. They all aim at preventing bacterial attachment and biofilm formation on medical devices and in body tissues and can be used in prevention or treatment and some in both applications. If successful the chance that an infection occurs is severely minimised. We collaborate in research and development but also open up research methodologies and biobanking facilities between partners. Slowly we are branching out our consortium and as a next step would like to extend the setup of our project to a new European DARTBAC structure. If successful we can save on short- and long-term healthcare costs and improve the population productivity. Also, our technologies can in time be applied worldwide. picture show some material developments within DARTBAC
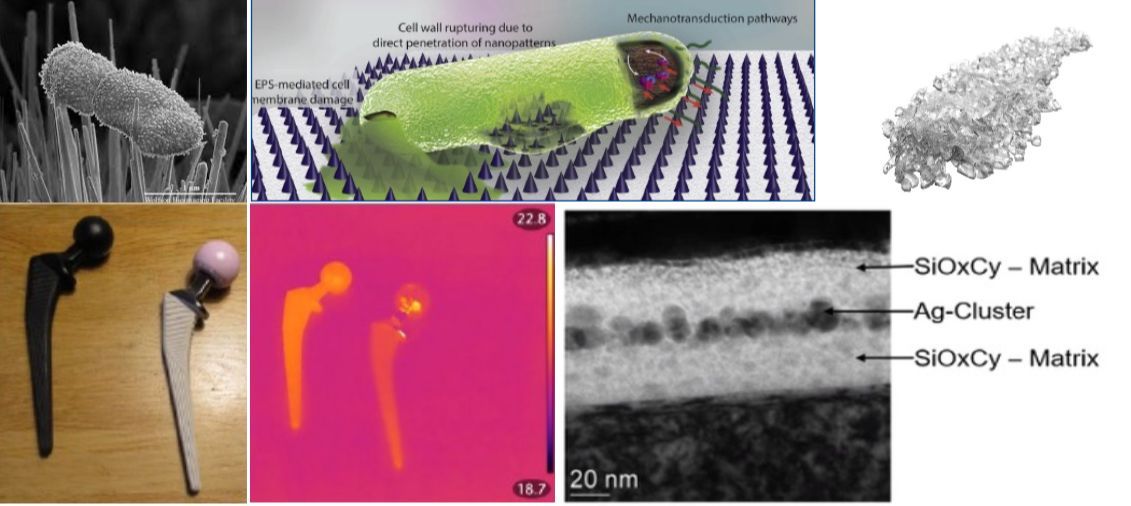
Top row: Left: 3-D printed spikes that have penetrated a bacterium.
Middle: Pyramid-shaped triangles that can damage the cell wall of bacteria.
Right: Bioactive glass that can have a bacteriostatic and bactericidal effect due to changes in pH and osmolarity. Bottom row: Left: Hip prosthesis without warming.
Bottom Middle: Thermal camera image of warmed hip prosthesis.
Right: Microscope image of a 3-layer coating with Silver as an active antibacterial component.
How worried should we be about Antimicrobial resistance?
We should be very worried. Prediction models tell us about 10M deaths will be related to AMR by 2050 and personally I believe that this is an underprediction. The associated healthcare costs for infection prevention and treatment and for the loss of productivity will be massive. Specifically for the United States, the Centres for Disease Control and Prevention (CDC) estimated the annual cost of AMR to be $55 billion - $20 billion for healthcare costs and $35 billion for loss of productivity. It is apparent that increases in antibiotic resistant bacteria will result in an higher infection incidence across all surgical interventions. These antibiotic-resistant bacteria will in future also be harder to eradicate. A combined higher incidence of infection by more antibiotic-resistant bacteria can result in higher treatment failure rates and ultimately increased incidence of complications and the necessity of amputations. It seems unlikely that the low infection incidence in primary joint arthroplasty results can be maintained in the next decades also warranting more revision surgeries and high associated healthcare costs.

What are you hoping to achieve with DARTBAC?
For the general population, we would like to establish more information about the threat of AMR. It will not stop at the border. Even more problematic, we cannot fully stop its development, only minimise its impact. Research that we perform should lead to new material technology able to prevent or kill antimicrobial resistant bacteria. The development of new high-speed diagnostics is also essential. I hope to extend the DARTBAC community to an European level.
How do you see the long term solution?
Well material technology and better diagnostics will help in mitigating AMR but not fully. New antibiotics or replacement pharmaceuticals are also desperately needed. For current antibiotics maybe local administration instead of systemic should be executed more, were possible of course. Governments,subsidy providers and policymakers need to be aware of the timelines of antibiotic and material technology developments and time to market approval. The investments on AMR are not sufficient and severely need to be increased. This requires a global approach as was performed during COVID and we each have a role to play.

How can we learn more about DARTBAC?
Well material technology and better diagnostics will help in mitigating AMR but not fully. New antibiotics or replacement pharmaceuticals are also desperately needed. For current antibiotics maybe local administration instead of systemic should be executed more, were possible of course. Governments,subsidy providers and policymakers need to be aware of the timelines of antibiotic and material technology developments and time to market approval. The investments on AMR are not sufficient and severely need to be increased. This requires a global approach as was performed during COVID and we each have a role to play.
Through our papers, social media channels and project website
linkedin.com/company/dartbac/
Youtube
youtube.com/@nwadartbac
Project website
https://nwa-dartbac.eu
Professor. Chris Arts

Chris Arts is Professor of Translational Biomaterials at the TU/e research group Orthopaedic Biomechanics and at the Maastricht University Medical Centre where he together with Prof Tim Welting heads the Laboratory for Experimental Orthopaedics. His clinical research focuses on translational biomaterials for delayed bone healing, infection treatment and spine deformity correction. This entails both the mechanical and biological assessment of biomaterials safety and efficacy performance but also longitudinal metabolic changes in the body. Utilizing high-resolution imaging combined with computational modeling the incorporation, remodeling and resorption phase of the biomaterials with the host tissue can be assessed. Furthermore assessment of bone healing in clinical patients; and evaluation and implementation of 3-D printing materials science and technology is a focus area. At Eindhoven University of Technology the focus of Arts' research is in assessment of contribution to mechanical bone strength of biomaterials during incorporation, remodeling and resorption phase using image analysis and validation and Finite Element Analysis (FEA). He aims at building bridges on biomaterials between medicine, clinical imaging and materials engineering research.
Read more about Professor. Art's practice here
We would like to thank Professor. Art's for his time and insight into orthopaedic excellence.
Thank you to our sponsors:



To download this issue of On The Podium, click below.
Sign up to On The Podium. The latest insights and inspiration from orthopaedic specialists around the globe sent straight to your inbox.
On The Podium
The newsletter brought to you by OrthoSpaceX
| Engage with Orthopaedic Leaders | Exclusive orthopaedic insight | |
| Stay Ahead in Orthopaedic Advancements | Uncover Surgical Innovations | |
| Empower Your Orthopaedic Knowledge | Unlock the Minds of Orthopaedic Specialists |